
Almost half of all heart attacks and strokes occur in people with none of the four classic modifiable risk factors: high blood pressure, high cholesterol, smoking, or diabetes. That gap has frustrated cardiologists for decades – and the explanation that’s emerging from recent research is not a new risk factor but a hidden biological process that standard checkups still rarely measure.
The answer is cardiovascular inflammation. Not the kind that comes with a fever or a sprained ankle, but a slow, chronic immune response quietly unfolding inside arterial walls – invisible to standard cholesterol panels, undetected by blood pressure cuffs, and measurable only with tests most doctors still don’t routinely order.
New data from Novo Nordisk’s POSEIDON study, presented at the 94th European Atherosclerosis Society Congress in Athens, Greece, confirms that a significant portion of patients with cardiovascular disease continue to face high inflammatory markers despite being on standard-of-care treatments. The findings don’t just fill a scientific gap. They challenge the assumption, widely held by both doctors and patients, that getting cholesterol and blood pressure under control is enough.
What Cardiovascular Inflammation Actually Does
Cardiovascular inflammation is an independent risk factor for events such as heart attack and stroke in people living with cardiovascular disease – meaning it operates separately from cholesterol, blood pressure, and everything else that standard care is designed to treat.
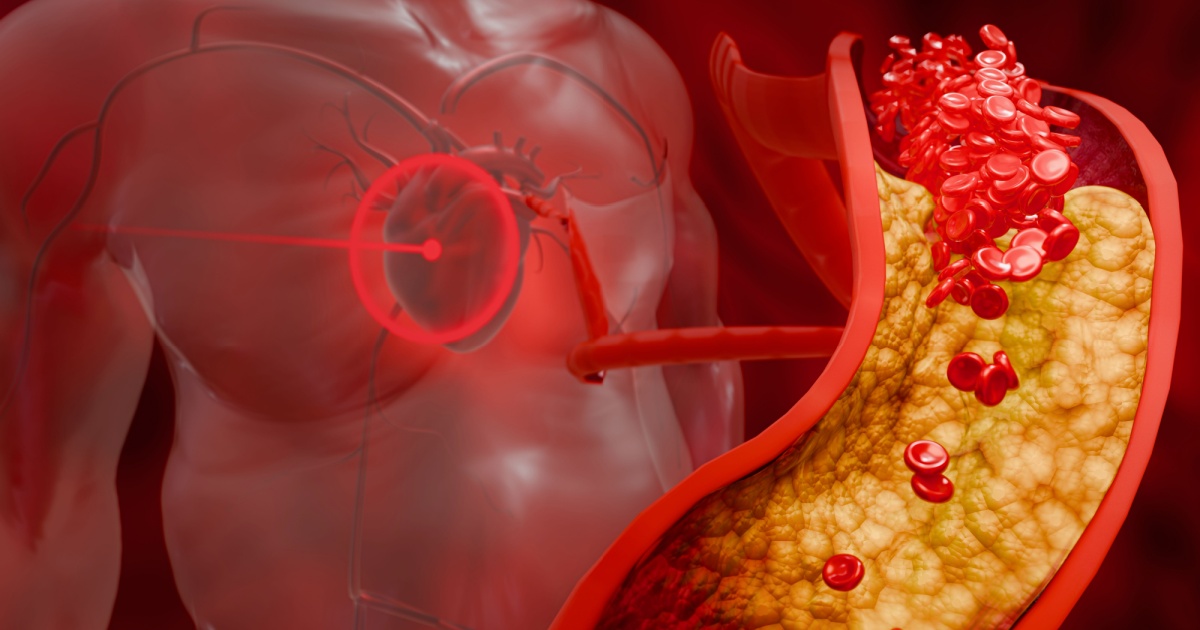
The mechanism isn’t abstract. Even a small accumulation of cholesterol inside the heart’s arteries provokes the immune system. The resulting immune response covers the plaque with a fibrous cap, but the smoldering inflammation underneath can cause that cap to rupture. The contents then mingle with blood, forming a clot – and those clots are responsible for most heart attacks and strokes.
Chronic inflammation – a prolonged, body-damaging state of immune system activation – may be the hidden factor that accelerates cardiovascular problems to a dangerous and deadly state. When cholesterol builds up in the arteries, it shape-shifts into a form the body no longer recognizes, prompting the immune system to attack both the cholesterol and the surrounding blood vessels. The damage that process leaves behind ends in heart attacks and strokes.
For people already living with heart disease, elevated hsCRP levels are as predictive of future heart attack and stroke as elevated LDL cholesterol – even in those taking statins. The POSEIDON real-world evidence study, which analyzed 18,904 patients across 18 countries, found that 2 in 5 individuals living with atherosclerotic cardiovascular disease, chronic kidney disease, or heart failure exhibit persistent inflammation – defined using high-sensitivity C-reactive protein (hsCRP) levels of 2 mg/L or higher.
The Test Most Doctors Still Don’t Order
Cardiovascular inflammation is measured through a blood test for hsCRP – a protein the liver produces in response to inflammation. An hsCRP result lower than 1 mg/L means lower risk; 1 to 3 mg/L indicates average risk; and 3 mg/L and up signals higher risk for cardiovascular disease, heart attack, and stroke. Despite the test being inexpensive and widely available, most people aren’t tested for inflammation unless they already have heart disease or another diagnosed inflammatory condition.
The growing recognition of the role of inflammation in cardiovascular disease is reflected in recent guidelines from the European Society of Cardiology, the American Heart Association, and the American College of Cardiology, which include elevated hsCRP as a risk-modifying biomarker to guide more intensive preventive initiatives. The ACC has called for universal screening with a high-sensitivity C-reactive protein test, and most insurers cover it. If your annual checkup doesn’t include hsCRP, ask your doctor to add it to the panel.
Lp(a): The Cholesterol Test Most People Have Never Heard Of
Cardiovascular inflammation is one part of the hidden risk picture. Another piece – equally underdiagnosed – is a specific type of cholesterol-carrying particle called lipoprotein(a), or Lp(a). Elevated Lp(a) levels are predominantly inherited and can raise cardiovascular risk even when traditional cholesterol levels are normal. Approximately one in five people has high Lp(a), and most are unaware because it usually does not cause symptoms. That combination – genetic, silent, and invisible on a standard lipid panel – makes it one of the most consequential risk factors that most adults have never been given reason to think about.
Research published in the Journal of Lipid Research in May 2025, led by Dr. Robert S. Rosenson at the Icahn School of Medicine at Mount Sinai, found that patients with high Lp(a) carry and express more tissue factor – the key regulator of blood clotting from the arterial wall – on their monocytes. That tissue factor activates blood clotting, which can lead to a heart attack. This is a mechanistic finding, not yet confirmed in a randomized controlled trial, but it provides a credible biological explanation for why high Lp(a) patients tend to experience acute cardiac events with little prior warning.
After nearly 4 years of follow-up, patients with Lp(a) above 175 nmol/L were 31% more likely to experience a major adverse cardiovascular event – a risk driven by elevated rates of stroke and cardiovascular death, but not heart attack. Those figures come from an observational analysis of previously collected plasma samples from 20,070 participants aged 40 and older across the ACCORD, PEACE, and SPRINT NIH randomized trials, presented at the Society for Cardiovascular Angiography and Interventions (SCAI) 2026 Scientific Sessions and the Canadian Association of Interventional Cardiology Summit in Montreal. The data has been presented at the conference stage and has not yet appeared in a peer-reviewed journal, but the scale of the sample adds considerable weight.
The findings reinforce the risks associated with elevated Lp(a) and strengthen recommendations for measuring it, including those from the most recent ACC/AHA dyslipidemia guidelines – which consider Lp(a) a risk-enhancing factor at levels of 125 nmol/L and higher, indicating that such levels should prompt more intensive lowering of LDL cholesterol and management of other risk factors. The American Heart Association’s Lp(a) guidance now states that every adult should have this test done at least once in their lifetime.
The Kidney Connection
The POSEIDON study found that 2 in 5 individuals living with atherosclerotic cardiovascular disease and chronic kidney disease exhibit persistent inflammation. That overlap matters because the relationship runs in both directions: inflammation contributes to chronic kidney disease (CKD) progression, and CKD itself promotes inflammation, creating a cycle that amplifies cardiovascular risk well beyond what standard calculators capture.
A large-scale study unveiled at the European Stroke Organization Conference (ESOC) 2026, analyzing over 460,000 participants from the UK Biobank, has also shed new light on how commonly overlooked physiological markers connect to cardiovascular danger. Anyone managing CKD should be asking their cardiologist whether their cardiovascular inflammation has been specifically measured, not assumed to be controlled by standard kidney or heart medications.
Atrial Fibrillation, Resting Heart Rate, and Silent Risk
Cardiovascular inflammation doesn’t operate alone. Several other under-recognized factors amplify stroke and heart attack risk in ways that often go undetected until an event occurs.
Patients with atrial fibrillation (AF) – an irregular heart rhythm – carry a 3 to 5-fold increased risk of stroke, and AF-related strokes tend to be more severe than those unrelated to the condition. AF is frequently paroxysmal, meaning it comes and goes, and many people have it without knowing. Implantable loop recorders can detect atrial fibrillation episodes to prevent stroke, and modern wearables can now catch episodes that a standard ECG would miss entirely.
Resting heart rate data from a 2026 UK Biobank analysis, presented at the European Stroke Organization Conference, found that stroke risk was lowest at rates of 60 to 69 beats per minute but increased at both extremes. At these extremes, stroke risk was 25% higher in those with very low heart rates and 45% higher in those with very high heart rates – a relationship that remained after adjustment for established stroke risk factors including hypertension, diabetes, and atrial fibrillation. These are observational findings, and the researchers note that resting heart rate may reflect underlying cardiovascular dysfunction rather than cause stroke directly. Even so, very low or very high heart rates should act as a signal for clinicians to look more closely at an individual’s overall cardiovascular risk.
Obstructive sleep apnea adds another layer of risk that most cardiovascular assessments ignore. A 2013 meta-analysis published in the International Journal of Cardiology – still among the most frequently cited studies on this topic – found that severe obstructive sleep apnea is associated with a more than 2-fold increase in the risk of fatal and non-fatal stroke. People with untreated sleep apnea who haven’t been evaluated for cardiovascular risk are likely operating with an incomplete picture of their actual vulnerability.
For people already managing heart disease, silent ischemia – reduced blood flow to the heart that produces no chest pain or other symptoms – is another factor worth raising with a cardiologist. According to data from the Journal of the American College of Cardiology, silent ischemia is associated with a substantially higher risk of adverse cardiovascular events, a striking figure given that it produces no warning signs by definition.
Metabolic Syndrome: The Quiet Multiplier
Metabolic syndrome is the cluster of conditions that includes central obesity, high blood pressure, high triglycerides, low HDL cholesterol, and elevated blood sugar. People who meet the criteria for metabolic syndrome carry roughly double the risk of atherosclerotic cardiovascular disease and five times the risk of developing diabetes, according to research published in Circulation. The prevalence of this cluster in the general adult population is high enough that many people carrying the combined risk don’t realize they qualify.
The connection between metabolic syndrome and cardiovascular inflammation is direct. Excess visceral fat – the fat stored around internal organs – is metabolically active. It releases inflammatory signals that elevate hsCRP and other inflammatory markers. Treating metabolic syndrome isn’t just about managing glucose or blood pressure; it also reduces the chronic inflammatory state those conditions generate.
Read More: Dietary Habits Driving Heart Disease Deaths
What to Do Now
Three blood tests are rarely ordered during a standard annual physical, but together they cover the most significant hidden cardiovascular risks identified by current research: an hsCRP test (ideally high-sensitivity), an Lp(a) level, and – if you have any unexplained symptoms like palpitations, fatigue, or breathlessness – a cardiac rhythm monitor or extended Holter monitoring to screen for paroxysmal atrial fibrillation.
“We should be testing people for CRP along with cholesterol in their 30s and 40s so we can intervene earlier in life,” according to Dr. Paul Ridker, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital. If your hsCRP comes back at 2 mg/L or higher and you’re already on a statin, ask your doctor whether you’re a candidate for low-dose colchicine (0.5 mg daily) – the first FDA-approved anti-inflammatory therapy proven to reduce heart disease risk when added to statin therapy.
Beyond medications, consistent physical activity of around 150 minutes per week, maintaining a healthy weight, prioritizing sleep, and eating a diet rich in whole, minimally processed foods are all associated with lower inflammatory markers and reduced cardiovascular risk. These targets directly lower hsCRP – the same marker that clinical research is now using as its primary measurement of cardiovascular danger. If your numbers stay elevated despite those changes, that’s the signal to push for a more targeted treatment conversation with your cardiologist.
Disclaimer: This information is not intended to be a substitute for professional medical advice, diagnosis, or treatment and is for information only. Always seek the advice of your physician or another qualified health provider with any questions about your medical condition and/or current medication. Do not disregard professional medical advice or delay seeking advice or treatment because of something you have read here.
AI Disclaimer: This article was created with the assistance of AI tools and reviewed by a human editor.
Read More: How to Spot Chronic Inflammation: 6 Key Symptoms and Solutions