
Most heart attacks start with an issue that initially hides in plain sight. Plaque can sit inside an artery for years, then suddenly crack and trigger a clot. Doctors can lower LDL and control blood pressure, yet they still struggle to spot which plaques will eventually become dangerous. Many scans can reveal how narrow an artery is, but they often miss what matters most inside the wall: inflammation, stressed immune cells, and unstable plaque structure. This is where nanoparticles enter the story. Researchers are now designing them as tiny, targeted tools that move through the blood with a specific purpose.
Some nanoparticles attach to inflamed plaque; therefore, imaging can highlight any potential risk much sooner. Others enter plaque macrophages and force cholesterol out of trapped cells. Some aim to restart the cleanup process that fails when dead cells build up. Teams at SAHMRI, Michigan State University, and Stanford-linked groups have already tested these ideas in animals and used imaging to prove the particles reached plaque tissue. Human proof still lies ahead, but the goal is clear: find the most dangerous plaque early on and then hit it directly instead of treating the whole body the same way.
Rupture Risk Is Not About Narrowing
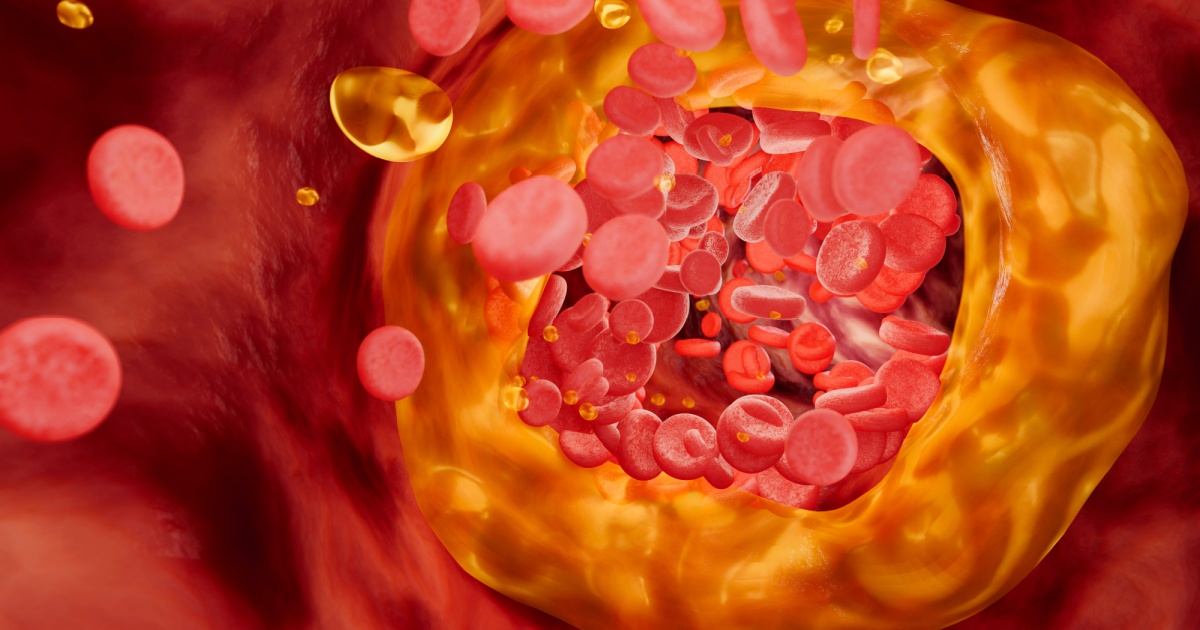
Atherosclerosis is often described as clogging, yet many heart attacks do not start at the tightest blockage. The highest-risk plaques are inflamed and fragile. They may sit under a thin fibrous cap that can tear, exposing a thrombogenic core to blood. In minutes, a clot can grow large enough to choke the flow through a coronary artery. This explains why cardiology is focusing on plaque biology, not only the percent of narrowing on an angiogram. Standard CT angiography can estimate plaque burden, yet it does not always reveal immune activity that predicts rupture. FDG-PET can capture inflammatory metabolism, but it is not routinely used for coronary screening, and its resolution can be limited. Michigan State University engineer Bryan Smith captured the public confusion when he said, “There are two different things that people seem to be scared of when it comes to plaques.
Many people don’t really understand the difference between them.” In the same MSU report, Smith called the inflammatory kind “the scarier one that leads to most heart attacks,” because it may not block much of the artery before rupture, and the blockage can appear suddenly after the tear. That gap between what looks severe and what behaves dangerously is the opening that nanoparticles try to exploit. If a particle can home in on macrophages, oxidized lipids, or other plaque signals, it can help clinicians find the lesions that require aggressive treatment even when the artery still appears passable. The ambition is practical: detect a risky plaque earlier, then deliver therapy directly into its immune hotspot, while leaving the rest of the body largely untouched.
A Particle Built for Macrophages
Researchers at the South Australian Health and Medical Research Institute designed porphyrin-lipid nanoparticles, or Por-NPs, to interact with macrophages inside plaque. Por-NPs are lipid-based particles that incorporate porphyrin-lipid in their shell. That chemistry matters because it supports near-infrared fluorescence, and it can chelate radionuclides such as Copper-64 for PET imaging, allowing one particle to reveal where it goes over time. The outside also carries a short peptide called R4F, which helps the particle engage receptors expressed on plaque macrophages and influences pathways tied to cholesterol handling and inflammation. In the peer-reviewed report describing the system, the authors summarize the core mechanism in one line: “Por-NPs are internalized by macrophages, promote cholesterol efflux and inhibit inflammation.” SAHMRI framed the same concept in everyday language. Dr Victoria Nankivell said, “These nanoparticles don’t just detect arterial plaque in arteries, they can also suck it up and take it to the liver, lowering inflammation.”
She also emphasized the cellular focus, noting that “What sets these nanoparticles apart is their ability to interact directly with immune cells in the arteries, drawing out cholesterol and helping the body process it more effectively.” The liver detail is important because it points to a biological exit route. If macrophages can offload cholesterol and the body can route it for processing, plaque biology can shift without relying on high systemic drug levels. This is the core promise of targeted nanoparticles: change the disease where it lives, inside the artery wall, with less collateral exposure elsewhere. In early testing, the particles also function as tracers, so researchers can confirm delivery and adjust the design based on where the signal accumulates and where it does not.
Lighting Up Plaque Biology
One reason plaque remains difficult to manage is that arteries hide their most relevant details. The lesion sits within a living wall, not on an exposed surface. Por-NPs were built to help with this problem by offering multiple ways to generate a signal. The SAHMRI paper explains that the porphyrin-lipid shell enables near-infrared fluorescence, and chelation with Copper-64 enables serial PET imaging. Those two modalities complement each other. PET can quantify signal deep within tissue, while fluorescence can provide high-resolution local confirmation in experimental settings. Because these nanoparticles are internalized by macrophages, the signal can act as a map of immune activity, not simply a map of vessel shape. A separate Scientific Reports study exploring HDL-like porphyrin nanoparticles described how the particles reach plaque through microvessels and dysfunctional endothelium.
The authors wrote that “Once infused, the nanoparticles enter the plaque through microvessels that extend into the plaque from the arterial adventitia,” and they noted that the lipoprotein-like structure gives an “extended circulation half-life” that supports detection after administration. This matters because circulation time is a make-or-break feature. A particle that disappears too quickly cannot reliably find plaque. A particle that lingers can deliver more signal, or more drug, at the site of interest. For future clinical use, imaging could also help triage. A clinician might use nanoparticle-enhanced PET to identify a patient with high inflammatory plaque activity, then intensify therapy and monitor whether the signal falls after treatment. Even if the first clinical role is diagnosis, the same platform can guide iterative design, because researchers can measure delivery instead of guessing.
Lower Inflammation, Move Cholesterol Out

In the SAHMRI-led study, Por-NPs were not treated as passive imaging agents. The team tested whether they could change macrophage behavior in ways that slow plaque growth. In vitro, the authors report that Por-NPs increased cholesterol efflux from macrophages and reduced inflammatory gene expression. That combination targets two connected drivers of plaque progression. When macrophages fail to export cholesterol, they become foam cells and amplify inflammatory signaling. When inflammatory pathways activate, they recruit more immune cells, stimulate cytokines, and can destabilize the lesion. A therapy that addresses both steps has a plausible route to lowering risk. The paper’s results section describes inhibition of inflammatory mediators that are commonly tied to atherosclerosis biology, including IL-1β and IL-18, plus chemokines such as CCL5.
It also reports suppression of NF-κB signaling, a major transcriptional driver of inflammatory gene programs in macrophages. In vivo, the authors describe plaque localization using PET and fluorescence, and they report smaller plaques in mouse models after Por-NP infusions. SAHMRI’s release translates that point into a treatment goal, stating that the nanoparticles “target inflamed plaques and significantly reduce both plaque size and inflammation.” Taken together, the claim is not that nanoparticles scrub arteries clean overnight. The claim is narrower and more testable: targeted particles can shift macrophage function inside plaque so that less cholesterol stays trapped and fewer inflammatory signals keep the lesion active. This approach also fits with real-world care. Statins lower circulating LDL, yet they cannot directly program plaque macrophages. A macrophage-directed infusion could, in principle, add benefit on top of existing therapy.
Turning Cleanup Back On
Another nanoparticle strategy focuses less on cholesterol export and more on cleanup. In advanced plaques, dead and dying cells accumulate and form a necrotic core. Macrophages are supposed to remove this debris through efferocytosis, yet that process becomes impaired as plaques mature. The Nature Communications study led by teams including Stanford and Michigan State University describes efferocytosis as a translational target and explains why CD47 became central. In the abstract, the authors state, “Reactivation of efferocytosis, the phagocytic removal of cells by macrophages, has emerged as a translational target for atherosclerosis.” CD47 acts as a “don’t-eat-me” signal. Blocking it systemically can boost clearance, yet it can also create serious side effects because red blood cells carry CD47 too.
The same abstract spells out the safety problem: “Systemic blockade of the key ‘don’t-eat-me’ molecule, CD47, triggers the engulfment of apoptotic vascular tissue,” but “it also induces red blood cell clearance, leading to anemia.” To avoid that trade-off, the group developed a macrophage-targeted nanotherapy that delivers a small-molecule inhibitor downstream of the CD47 pathway, aiming to boost efferocytosis primarily in plaque monocytes and macrophages. They describe the particle as a “‘Trojan horse’ nanoparticle” that selectively delivers the drug to inflammatory monocytes and macrophages within plaque. This mechanistic framing matters for clinical translation. It offers a safety rationale that regulators will demand: the therapy aims to confine pro-efferocytic action to the lesion’s immune cells, while avoiding widespread effects on blood cells. If that selectivity holds in humans, it could reduce necrotic core growth and lower rupture risk without forcing clinicians to accept anemia as the price.
Why Pigs Matter
Mouse studies can show a mechanism, yet human arteries behave more like large-animal arteries in size, flow, and plaque complexity. That is why the MSU and Stanford collaborators moved their nanotherapy into a porcine model. The Nature Communications paper reports that the nanoparticle could be produced at a larger scale and still function, and that treatment reduced inflammation in lesions at an early stage of disease without inducing anemia. That last point is not a marketing detail. It is a central safety gate, because earlier CD47-blocking approaches can trigger anemia through non-specific red blood cell clearance. The MSU Innovation Center report also highlights the imaging angle in pigs. Smith explained how the team quantified response, saying, “Using PET scans, we were able to measure the effects of the therapy on pig arteries.”
He added that the group showed they could decrease plaque inflammation using PET alongside molecular assays, and he emphasized the safety readout: “Just as importantly, we saw none of the side effects that would have been anticipated had the therapy not been precisely targeted.” New Atlas quoted Smith describing the same pig work, reinforcing that the study used clinically familiar imaging tools while testing a targeted biological therapy. Large-animal evidence does not guarantee human success, but it reduces the risk that a therapy only works in a small rodent model. It also forces practical decisions about infusion dose, particle stability in blood, and measurement methods that resemble real clinical workflows. Those steps are often where promising nanomedicine fails, so passing them is meaningful even before any human trial begins.
The Engineering That Makes or Breaks It
Nanoparticles succeed or fail because of design choices clinicians never see. Size controls where particles travel in the body. Surface charge affects protein binding and how fast the body clears particles. Coatings also decide whether immune cells remove particles before they reach plaque. A Scientific Reports paper on HDL-like porphyrin nanoparticles highlights a key advantage. The authors say the lipoprotein-like design “enables them to evade the immune system.” That design also gives an “extended circulation half-life,” which can reduce the need for PEGylation. The same paper explains why PEGylation can create problems. PEGylation can reduce cell uptake and raise concerns about anti-PEG immune responses.
Scale creates another hard barrier. A therapy can work in mice with tiny doses and still fail later. Production must reach liters for large animals and future human trials. A Nature Communications pig study emphasized this point clearly. The authors wrote, “We demonstrate that production can be scaled without impairing nanoparticle function.” The MSU report adds a practical detail about dose scale-up. Earlier mouse work used hundreds of microliters. The team then scaled production to liters for pig studies. That shift moves the platform closer to human use. These details may sound technical, yet they decide what reaches patients. Manufacturers must produce identical batches every time. They must sterilize and store the product without damage. Clinicians must infuse it safely and predictably. Repeat dosing raises the bar even higher. Long-term tolerance must stay strong across many doses. Batch consistency must also remain reliable over time.
Where This Fits in Treatment
Nanoparticle plaque therapies will not replace standard heart care. Doctors will still rely on statins and blood pressure control. They will still push smoking cessation and diabetes control. They will still use antiplatelet therapy when it fits the patient. The key question remains practical. Can a targeted infusion cut risk in patients who remain high-risk? A 2025 Biomedicines review says atherosclerosis involves chronic inflammation and major risk of death. It also says residual risk and treatment limits “underscore the need for innovative strategies.” Clinicians will demand clear trial goals before they adopt this approach. Imaging can support decisions, yet outcomes will decide the value. Doctors will look for fewer heart attacks and strokes. They will track fewer hospital stays and fewer procedures.
Early trials will focus on safety and how the body handles the infusion. Teams will measure drug levels and basic biomarkers. They will also measure changes in plaque inflammation on scans. The MSU and Stanford pig work already used PET scans for this purpose. The teams also watched for anemia during treatment. Por-NPs could support a different clinical flow. Doctors could use them as tracers and as treatment tools. They could identify macrophage-rich plaques, then confirm dose delivery. Clinicians might add an infusion for patients with repeat events. They might also target patients with high inflammation signals on imaging. The next step requires strict trials that prove benefit and avoid new harms.
Conclusion

Nanoparticle plaque research is shifting from theory toward real cardiovascular treatment. Studies from SAHMRI, MSU, and Stanford follow a shared strategy. Researchers target plaque macrophages to change the biology that makes plaques dangerous. The goal is to remove cholesterol, reduce inflammation, and restore proper cleanup inside plaques. Animal studies show lower plaque inflammation and, in some cases, smaller plaque size. Imaging signals also confirm that nanoparticles reach their intended targets.
The evidence remains preclinical, and no human trials indicate fewer heart attacks yet. No study can confirm long-term safety with repeated dosing in people. Researchers stress clear limits alongside progress. Dr Victoria Nankivell explained that inflammation drives plaque growth, and nanoparticles aim to break that cycle. Bryan Smith emphasized that precise targeting helped avoid expected side effects in pigs. The next phase requires strict safety testing, controlled manufacturing, and outcome-focused trials. Imaging and clinical results must guide progress, not excitement or headlines. If those steps succeed, nanoparticles could become reliable tools against dangerous plaque. For now, the concept looks sound, the data show promise, and the work ahead remains demanding and measurable.
A.I. Disclaimer: This article was created with AI assistance and edited by a human for accuracy and clarity.
Read More: Subtle Heart Attack Symptom Many Women Miss Without Realizing